Influenza and ARVI: similarities and differences of the diseases
95%
ARVI and influenza are infectious viral respiratory pathologies accounting for up to 95% of infectious diseases.
200+
ARVI is caused by more than 200 types of viruses including the influenza virus being one of the most dangerous of them.1 The incidence of these diseases is registered globally all year round with the peak falling on the cold season.
Symptoms of influenza and ARVI

Both of the diseases can be recognized by the first signs. The differences between ARVI and influenza consist in the fact that the acute respiratory viral infection does not cause severe complications.
The influenza pathogen is constantly changing. It's a serious disease, which can cause severe complications2 both in adults and children.
Mode of infection

ARVI
Contact with an infected person or via household items; droplet spread.
INFLUENZA
Droplet spread from an infected person as a result of close contact, conversation, sneezing or coughing.
Disease onset

ARVI
Gradual augmentation of symptoms.
INFLUENZA
Sudden and severe feeling unwell.
Elevated body temperature

ARVI
Up to 38–38,5 °C for up to 3 days.
INFLUENZA
Higher than 39 °C with sudden increase for up to 5 days.
Runny nose

ARVI
Often appears from the first days of infection, sneezing.
INFLUENZA
Moderate nasal congestion manifests itself on day 2–3 . Sneezing is rare.
Sore throat

ARVI
Redness and soreness are pronounced and frequent. Appear at once.
INFLUENZA
Not always. Redness and soreness can appear on day 2–3 after the infection.
Cough

ARVI
Productive or non-productive, from the first days of infection.
INFLUENZA
Troublesome, accompanied by pain and cramping behind the breastbone.
Lymph node condition

ARVI
Enlarged.
INFLUENZA
Often not changed.
General well-being

ARVI
Drowsiness, severe fatigue. Occurs fast.
INFLUENZA
Rapid loss of strength.
Additional symptoms

ARVI
Headache, conjunctivitis, intestinal disorders are possible.
INFLUENZA
Insomnia, migraine attacks, redness of the sclera of the eyes, noise and congestion in the ears.
Disease development

ARVI
Symptoms develop slowly.
INFLUENZA
Symptoms appear at once, condition worsens rapidly.
Intoxication

ARVI
Symptoms are mild.
INFLUENZA
Symptoms augment rapidly and are expressed in chills, muscle, joint, head ache, photophobia, nausea, vomiting, and diarrhea.

What is the danger of influenza and ARVI?
291 000 — 646 000
people4
A full-scale study conducted by the US Centers for Disease Control and Prevention and WHO has revealed that 291,000–646,000 people die annually of influenza and its complications worldwide4. The disease affects mostly children, elderly people and those suffering from chronic diseases.
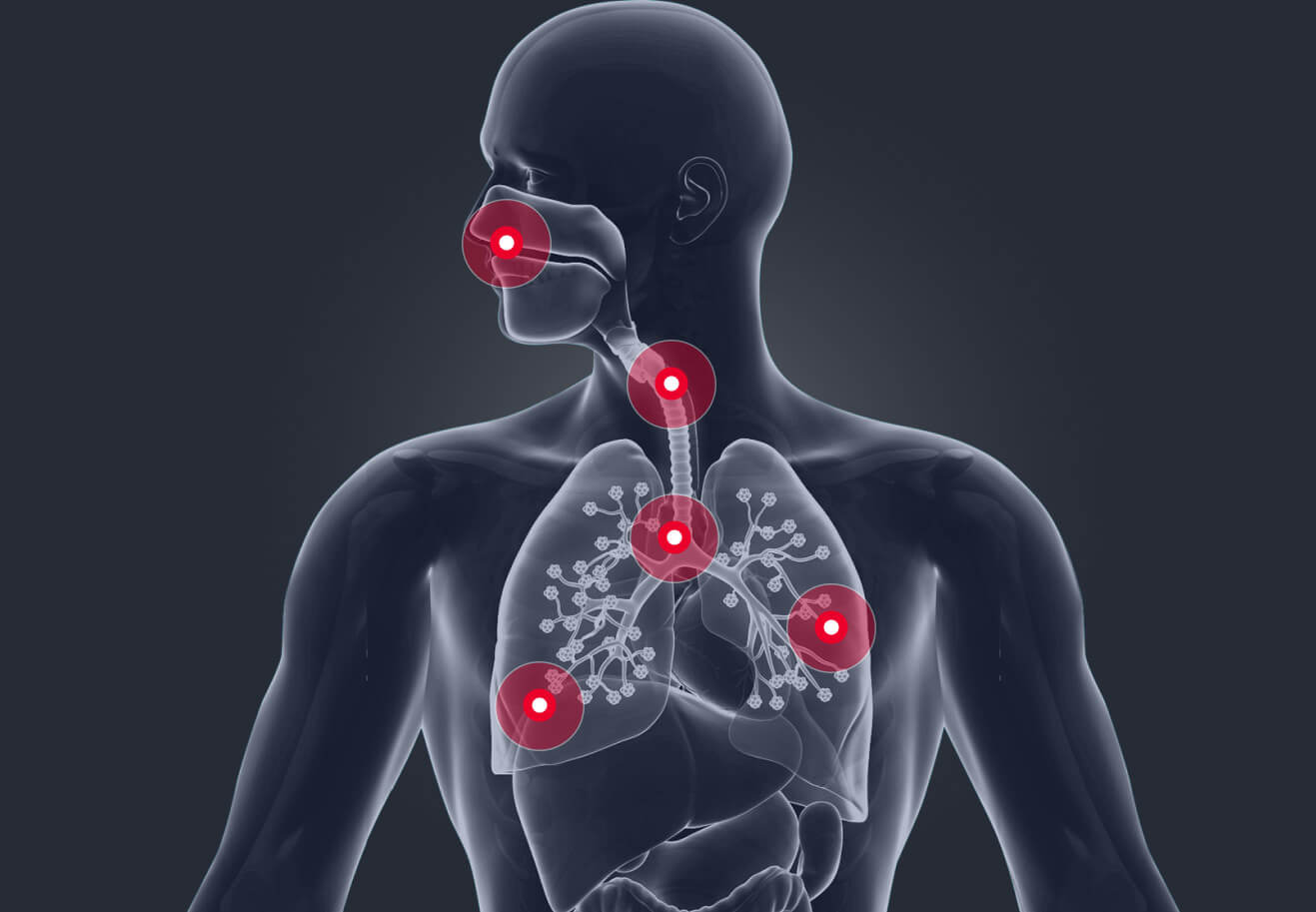
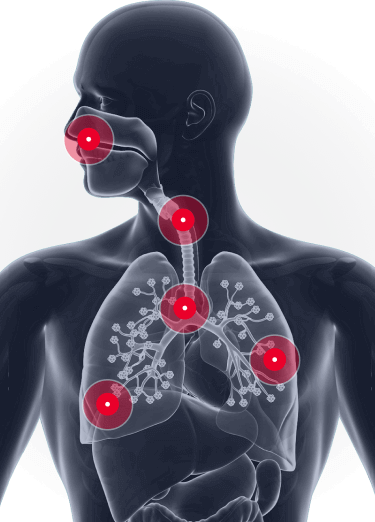
If influenza and ARVI are not timely treated, the inflammatory process will spread beyond the respiratory tract, invading other organs.
Virus spread infographics
Most frequent influenza and ARVI complications5
| BODY SYSTEM | DISEASES | OCCURRENCE RATE |
| Cardiovascular system | Myocarditis, pericarditis | Rare |
| Nervous system | Meningitis, meningoencephalitis, encephalitis, neuralgia, polyradiculoneuritis, Guillain-Barré syndrome | Rare, but severe |
| ENT-organs | Otitis, sinusitis, laryngitis, tonsillitis, sinusitis, rhinopharyngitis | Frequent |
| Respiratory organs | Tracheitis, bronchitis, pneumonia, acute respiratory distress syndrome, obstructive syndrome | Frequent |
| Kidneys | Glomerulonephritis | Rare, with severe consequences |

Modes of transmission

ARVI
The modes of transmission depend on the pathogen. In case with ARVI the virus is active for the transmission from one person to another for two hours! The “entrance gate” for acute respiratory viral infection is mucous membranes of the nose, mouth and eyes.
ARVI can be also transmitted via droplet spread or contact. An infected person touches a lot of objects within 2 hours, and other people can be infected at once by contacting the objects.
ARVI transmission modes
-
 Household items (dishes, towels, hairbrushes)
Household items (dishes, towels, hairbrushes) -
 Transport: handles, seats
Transport: handles, seats
-
 Indoors: door knobs, tables, chairs
Indoors: door knobs, tables, chairs -
 Crowded places
Crowded places
-
 Toys
Toys -
 Dirty hands (touching the face)
Dirty hands (touching the face)
-
 Personal belongings of the infected person
Personal belongings of the infected person

INFLUENZA
The situation with the influenza virus is different, since it is transmitted mainly by droplet spread. However, the virus is also transmitted via contact and household items.
The influenza virus remains viable for up to 21 days. The source of infection is an infected person, and in some cases the virus can be transmitted from animals to humans6.
Influenza transmission modes
-
 Droplet spread via sneezing, coughing, emotional conversation. The virus is transmitted with saliva and phlegm containing pathogenic flora.
Droplet spread via sneezing, coughing, emotional conversation. The virus is transmitted with saliva and phlegm containing pathogenic flora. -
 Via household items (bed sheets, dishes, toiletries, toys)
Via household items (bed sheets, dishes, toiletries, toys)

Influenza and ARVI prevention tips

The best protection against acute respiratory viral infections is your own immunity. Take care of the protective functions of your body in advance.
Polyoxidonium® can increase the body's resistance to viral infections8, boost immunity and reduce ARVI reoccurrence13.
Polyoxidonium® boosts immunity and reduces ARVI reoccurrence
- https://cyberleninka.ru/article/n/sovremennye-printsipy-diagnostiki-i-lecheniya-orv/upload/images/viewer
- http://cgon.rospotrebnadzor.ru/content/22/27/3120/
- https://eduherald.ru/ru/article/view?id=17378
- https://www.who.int/influenza/ru/
- https://mosgorzdrav.ru/ru-RU/news/default/card/3038.html
- https://www.rmj.ru/articles/bolezni_dykhatelnykh_putey/Ostrye_respiratornye_virusnye_infekcii_i_gripp_etiologiya_diagnostika_i_algoritm_lecheniya/
- https://www.who.int/ru/news-room/fact-sheets/detail/influenza-(seasonal)
- Patient information leaflet for Polyoxidonium®.
- Vavilova, V.P., Vavilov, A.M., Cherkayeva, A.Kh. (2015). Possibilities of modern therapy for acute respiratory viral infections in children. Pediatrics (Appendix to Consilium Medicum), 3.
- Karaulov, A.V., Gorelov, A.V. (2019). The use of azoximer bromide for treatment of inflammatory infections of respiratory system in children: a meta-analysis of controlled clinical studies. Journal of Infectology, vol. 11, No. 4, 31–41.
- Mavzyutova, G.A., Mukhamadiyeva, L.R., Fazlyeva, R.M., Mirsayeva, G.Kh., Tyurina, E.B. (2015). Rational immunotherapy in the combination treatment of community-acquired pneumonia. Medical Council, 16.
- Garaschenko, T.I., Karneeva, O.V., Tarasova, G.D., et al. (2020). Influence of local application of Polyoxidonium on symptoms and course of acute respiratory viral infection in children: results of multicenter double-blind placebo-controlled study. Consilium Medicum, 22(3), 80–86.
- Kharit, S.M., Galustyan, A.N. (2017). Azoximer bromide is a safe and effective drug for treatment of acute upper respiratory tract infections in children: an overview of the results of double-blind, placebo-controlled, randomized clinical trials of phase II and III. Pediatrics (Appendix to Consilium Medicum), 2.
- Morozova, S.V. (2010). The use of Polyoxidonium® immunocorrecting drug in acute infectious inflammatory pathology of ENT-organs. Russian Medical Journal, vol. 18, No. 24.